CONTENTS
- Health Regulations Need a Base to Top Approach
- Personal Law Norms and Inter-Faith Marriages
Health Regulations Need a Base to Top Approach
Context:
In the last week of May, a devastating fire at a private neonatal care nursing home in New Delhi shocked everyone. Political parties engaged in a blame game, and the media coverage was intense, sometimes inaccurately claiming that many nursing homes in Delhi operate without licenses. Despite the parents’ ongoing grief, the incident has largely faded from public memory. Such tragedies often prompt questions about who is to blame, overlooking the fact that they are usually the result of systemic failures—in this case, the failure of healthcare regulations.
Relevance:
GS2- Health
Mains Question:
Health regulations are essential but their implementation in India needs to be nuanced and calibrated. Analyse. (10 Marks, 150 Words).
Healthcare Regulations- Challenges:
Excess of Regulations:
- Regulation has always been a key concern for health program managers but is arguably one of the weakest aspects of India’s healthcare system.
- The issue isn’t a lack of regulations; in fact, there’s an excess. Some states require over 50 approvals under various regulations for every healthcare facility.
- Despite this, many officials and others believe that the private health sector in India is under-regulated.
Unrealistic Healthcare Quality Standards:
- Another challenge is the unrealistic healthcare quality standards. Both national and state governments in India are known for drafting nearly perfect policies that are impractical to implement.
- For example, the Clinical Establishments (Registration and Regulation) Act, 2010, though enacted 14 years ago, hasn’t been adopted by states due to its impractical provisions.
- Similarly, the Indian Public Health Standards (IPHS), first released in 2007 and revised twice since, are intended to ensure quality health services. However, in 17 years, only 15% to 18% of government primary healthcare facilities in India meet these standards.
- In striving to be aspirational, India’s healthcare regulations and standards have become unrealistic and difficult to implement.
Government Sector vis-à-vis Private Sector:
- India’s healthcare system is mixed, with a common misconception that the government sector consistently follows regulations while the private sector frequently violates them.
- In reality, private healthcare facilities and providers deliver nearly 70% of outpatient services and 50% of hospital-based services in India.
- States like Maharashtra and Kerala have better health indicators not due to exceptional government facilities, but because private sector clinics and facilities effectively meet people’s healthcare needs, demonstrated by the high usage of these services.
- However, when it comes to healthcare regulation, there appears to be a bias, with stricter enforcement on the private sector.
- For instance, in 2017, two similar incidents occurred in Delhi, where newborns were incorrectly declared dead by a government hospital and a private hospital. The private hospital faced a temporary suspension of its license, while the government hospital only faced an inquiry committee.
- Effective regulation should not make stakeholders feel unfairly targeted. Currently, the burden of compliance falls heavily on providers and facility owners.
- Many private nursing homes and clinics report significant delays in approval processes, even when applications for renewals are submitted well in advance.
- Often, approvals granted months later, despite timely applications, highlight the sluggishness of the system and remain a major concern for facility owners.
Role of the Private Healthcare in India:
- Affordable care is essential. The private sector in India is diverse, ranging from single-doctor clinics and small nursing homes to medium-sized and large corporate hospitals.
- Single-doctor clinics and small nursing homes often serve as the first point of contact for middle-income and low-income populations, providing a substantial share of health services at a fraction of the cost of large corporate hospitals.
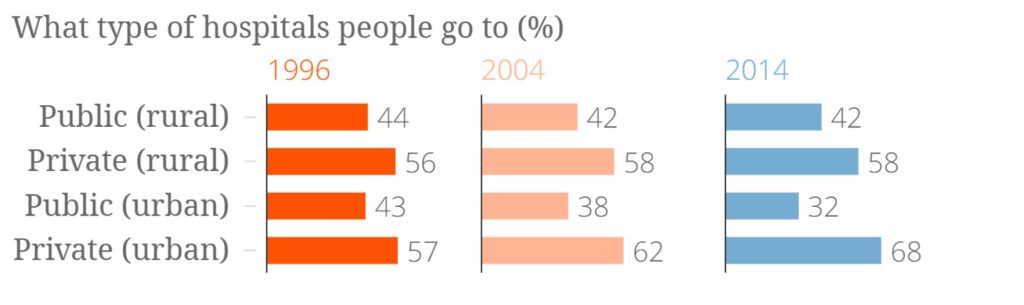
- The preference of parents for private nursing homes over free government health facilities highlights the importance of these smaller establishments in delivering accessible and affordable healthcare.
- Therefore, regulations should support and facilitate the operation of these smaller facilities to keep healthcare costs low.
Way Forward:
- The tragic incident in Delhi should prompt calm assessment and concrete planning. Ensuring quality health services is a joint responsibility of all stakeholders.
- While striving for world-class standards or catering to medical tourism, the government should avoid making healthcare regulations unrealistic.
- Practical and implementable guidelines are needed, along with harmonized health regulations and simplified application processes that are resolved in a timely manner.
- Moreover, regulations should consider the feasibility for different types of facilities. Imposing the same standards on smaller clinics and nursing homes as on large corporate hospitals would increase costs, which would likely be passed on to patients, making healthcare unaffordable.
- A differential approach with essential and desirable standards for each category, monitored through regular self-assessments and regulatory visits, is necessary.
- Just as buildings maintain safe elevators, health facilities should equally emphasize fire and safety measures. To improve adherence, the government should consider providing subsidies and funding.
- Furthermore, the process of forming regulations should involve representatives from doctors’ associations, relevant facilities, and community members.
- Lastly, political rhetoric and sensational media coverage can exacerbate public mistrust of doctors and nursing homes, potentially leading to increased violence against healthcare providers.
- Fifth, and most importantly, India needs to support and promote single-doctor clinics, smaller healthcare facilities, and nursing homes.
- These providers deliver primary care and help keep healthcare costs low. Every such facility and its doctors should be supported, not burdened with excessive regulations.
- The fire tragedy in Delhi underscores the need to address root causes, not just symptoms. Simplified and implementable regulations, developed through collaboration and coordination with key stakeholders, are essential.
- Fair implementation, time-bound decisions, and timely disposal of license renewal applications are crucial. Promoting smaller healthcare facilities with subsidies and support for improved quality and safety is also necessary.
Conclusion:
India’s healthcare system is increasingly skewed towards inpatient services. There is a need to promote providers and facilities that deliver cost-effective outpatient care. This aligns with the National Health Policy, 2017, which aims to provide people-centric, accessible, affordable, and quality health services. Achieving this requires health regulations to be drafted from the bottom up, implemented in a nuanced and calibrated manner.
Personal Law Norms and Inter-Faith Marriages
Context:
The principle that ignorance of the law is no excuse applies to both offenders and judges. This was evident in the Madhya Pradesh High Court’s ruling, which declined to protect a couple on the grounds that a marriage between a Muslim man and a Hindu woman would not be valid, even if registered under the Special Marriage Act (SMA), 1954.
Relevance:
GS1-Indian Society
GS2-
- Social Empowerment
- Judgements and Cases
Mains Question:
Personal law norms cannot be used to invalidate inter-faith marriages. Discuss in the context of recent judgements and rulings of the judiciary. (10 Marks,, 150 Words).
The Special Marriage Act of 1954:
About:
- The Special Marriage Act (SMA), 1954, is an Indian law that establishes a legal framework for marriages between individuals of different religions or castes.
- It governs civil marriages, sanctioned by the state rather than by religious authorities. This dual system, recognizing both civil and religious marriages, is similar to the UK’s Marriage Act of 1949.
Applicability:
The SMA applies to people of all faiths across India, including Hindus, Muslims, Sikhs, Christians, Jains, and Buddhists.
Recognition of Marriage:
- The Act allows for the registration of marriages, providing legal recognition and various legal benefits and protections, such as inheritance rights, succession rights, and social security benefits.
- It prohibits polygamy and declares a marriage void if either party had a living spouse at the time of marriage or if either party is incapable of giving valid consent due to unsoundness of mind.
Written Notice:
- Section 5 of the Act requires parties to give written notice to the Marriage Officer of the District, with at least one party residing in the district for at least 30 days before the notice.
- Section 7 allows any person to object to the marriage within 30 days of the notice’s publication.
Age Limit:
The minimum age for marriage under the SMA is 21 years for males and 18 years for females.
Differentiation from Personal Laws:
- Unlike personal laws such as the Muslim Marriage Act, 1954, and the Hindu Marriage Act, 1955, which require spouses to convert to each other’s religion, the SMA allows inter-faith or inter-caste marriages without requiring conversion.
- However, once married under the SMA, an individual is considered severed from their family concerning rights like inheritance.
More on the Recent Judgement:
- The judge referred to Muslim law treatises and concluded that a Muslim cannot marry an “idolatress or fire-worshipper,” deeming such a marriage irregular.
- However, the SMA was specifically enacted to allow inter-faith couples to marry without adhering to the religious rituals of their respective faiths.
- It is bizarre for a court to scrutinize the personal law requirements of the parties when they were merely seeking police protection to appear before the Marriage Registration Officer.
- The question about whether the inter-faith marriage intended to be registered under the SMA would be valid under Muslim law was completely irrelevant to the case.
The Court’s Argument:
- Despite the couple’s counsel correctly arguing that the SMA overrides the personal laws of their respective religions, the judge chose to determine the marriage’s validity, voidness, or irregularity under Mohammedan law.
- The judge acknowledges that a marriage performed under the Special Marriage Act (SMA) cannot be challenged for not adhering to mandatory marriage rituals.
- The only justification offered by the judge is that the SMA itself states that marriages within prohibited degrees of relationship are invalid.
- From this, he concludes that a marriage invalid under personal law cannot be legalized by registering it under the SMA.
- This provision is clearly intended to prevent the Act from being misused to solemnize marriages within prohibited relationships and does not imply that every inter-faith marriage must comply with personal law requirements.
- It is peculiar that the court highlights the woman petitioner’s refusal to convert to Islam while simultaneously evaluating the case through the lens of Muslim law. This approach attempts to impose religious personal law on those opting for a secular marriage.
Conclusion:
Allowing this judgment to stand would render the entire SMA redundant, undermine efforts towards a uniform civil code, and privilege Muslim personal law over the secular SMA. Essentially, it could drive people to religious conversion merely to solemnize their marriages.



